We often talk about front door control and back door control, right?
Original Zhao XI’s preface to Xi area This article is paid reading content, and paying users can give a friend a chance to read this article for free.
Cardiac CT scanning is an important achievement of CT development in recent 20 years. With the continuous progress of equipment, the fastest single sector time resolution has reached 66ms(SOMATOM Force). The improvement of time resolution is an important direction of CT development, and the most effective method is to improve the rotation speed of the gantry.
The earliest cardiac CT imaging mainly used ECG-gated technology, which retrospectively selected images in the relatively static position of heart movement and reconstructed them, so it was called retrospective ECG-gated scanning technology.
What is retrospective ECG-gated scanning technology?
Retrospective ECG-gating is what we usually call "back door gating". Retrospective ECG-Gating technology uses the synchronous acquisition technology of ECG and CT scanning to obtain the synchronous data of continuous spiral scanning and heart movement. After scanning, we can select any phase needed in the cardiac cycle according to the synchronized ECG for reconstruction.
According to the setting of CT scanner, the phase is defined as the percentage of relative-relative interval (such as 75%) or the absolute delay value (such as 700 milliseconds). (see:). It is known that the cardiac phase with the least motion artifacts is different between each coronary artery and the patient. Generally speaking, at low heart rate (i.e. < 65 bpm), coronary artery images with (almost) no motion are provided in the middle or late diastole. However, end-systolic reconstruction is necessary for a higher heart rate.
Searching for the best phase for each coronary artery from several phases (images are usually reconstructed with 5% R-R interval) is very time-consuming and requires great efforts. For automatic technology, "motion map" has advantages, which derives velocity function between multiple low-resolution reconstructions of cardiac cycle, and the minimum difference period between adjacent phases indicates the minimum cardiac motion.
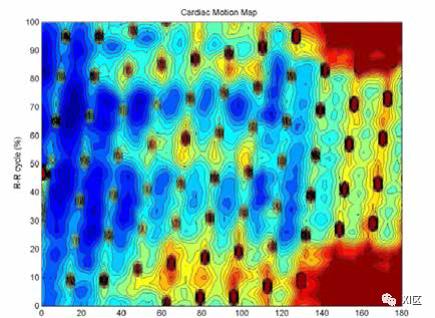
Cardiogram. The abscissa z shows the relative anatomical position of the heart, and the ordinate shows the position of adjacent images when the heart fluctuates. Blue indicates that the motion amplitude is small, and red indicates that the motion amplitude is large.
For images without cardiac motion artifacts, the acquisition time must be shorter than 19.1 milliseconds. Multi-slice spiral CT and electron beam CT do not have such high time resolution; Therefore, CT scanning imaging of the heart needs to properly adjust the scanning window to a relatively stable heartbeat phase.
According to Lu et al., by using ECG trigger/gating to optimize the cardiac phase, for a patient’s baseline heart rate of 50 to 100 beats per minute (bpm), a cardiac image with minimum motion can be obtained with an acquisition time of 50.9 to 75.5 ms..

Minimum and maximum velocity of three main coronary arteries in cardiac cycle (mm/s)
Lu B , Mao S S , Zhuang N , et al. Coronary artery motion during the cardiac cycle and optimal ECG triggering for coronary artery imaging. Investigative Radiology, 2001, 36(5):250-256.
In addition to coronary angiography, retrospective ECG gated scanning can evaluate global and local cardiac function (ejection fraction) and valve shape and function. Retrospective ECG gated scanning can adapt to patients with mild irregular rhythm.
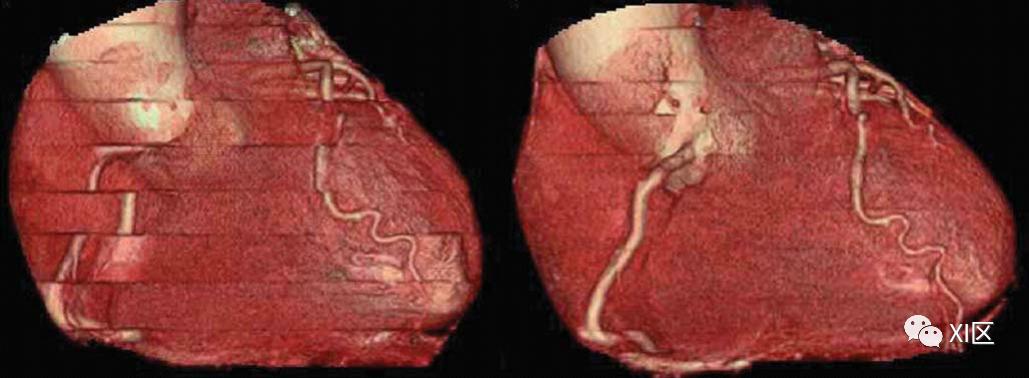
Electrocardiogram editing technology. The heart rate of patients with arrhythmia is 34-145 beats/min. In 75% of R-R reconstruction, obvious stepped (that is, banded) artifacts (left) are shown. Applying ECG editing technology (right) can reduce image registration errors.
Horiguchi J , Yamamoto H , Kihara Y , et al. Prospective ECG-triggered sequential versus retrospective ECG-gated spiral CT: Pros and cons. Current Cardiovascular Imaging Reports, 2009, 2(6):447-454.
Using ECG editing technology, the position of time window in cardiac cycle can be modified at will, and some or all artifacts caused by arrhythmia can be corrected and compensated. Therefore, by covering the data of the whole cardiac phase, retrospective ECG gated scanning can be used for multiple cardiac phase reconstruction and is robust enough for slight heart rate changes.
As an improvement of the traditional retrospective ECG-gated scanning, the current multi-row CT scanner has the so-called "ECG modulation" option, which modulates the tube current in a specific part of the cardiac cycle, allowing the radiation dose to be reduced by 30% to 50%.
The degree of reduction mainly depends on the setting of two parameters:
1) Percentage of minimum tube current/maximum tube current; and
2) The time length of the minimum tube current relative to the R-R interval.
For patients with low heart rate, systolic phase is usually not used for coronary angiography, and systolic phase can be selected as a window to reduce current. However, the low-dose data can reasonably evaluate the cardiac function, because such high image quality is not needed in the systolic phase of the heart in the above cases.
Prospective ECG trigger technology and retrospective ECG gating technology
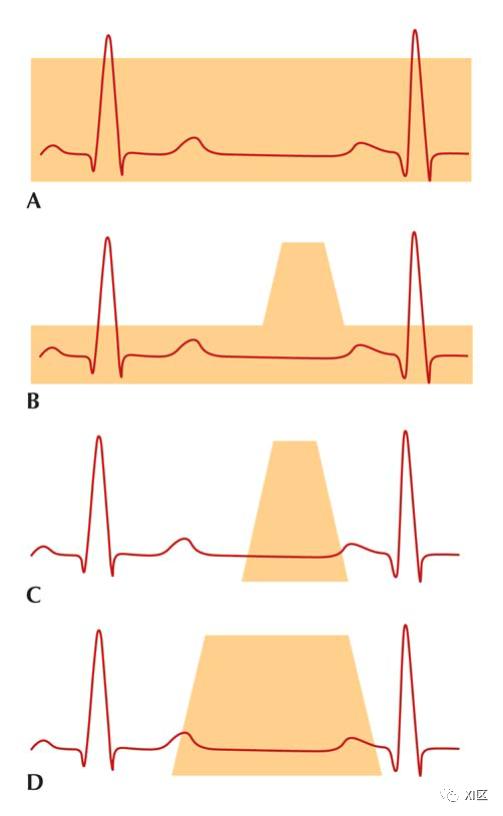
A. The traditional retrospective ECG gated scanning is carried out in spiral mode with fixed tube current during the whole cardiac cycle. B retrospective ECG-gated scanning with ECG modulation can reduce the tube current in a specific part of the cardiac cycle (usually during systole) and allow the radiation dose to be reduced by 30% to 50%. C. Prospective ECG trigger scanning applies radiation during a short and predetermined acquisition window of the cardiac cycle, thus reducing the radiation dose by about 80% compared with retrospective ECG gated scanning. D x-ray irradiation in prospective ECG trigger scan can be prolonged to increase additional reconstruction usability. It can regulate some heart rate variability; However, this is at the expense of increasing radiation exposure.
Horiguchi J , Yamamoto H , Kihara Y , et al. Prospective ECG-triggered sequential versus retrospective ECG-gated spiral CT: Pros and cons. Current Cardiovascular Imaging Reports, 2009, 2(6):447-454.
What is prospective ECG trigger scanning technology?
Prospective ECG trigger scanning technology can be traced back to more than 40 years ago. The new SOMATOM 2 equipment produced by Siemens Medical in 1979 can image the beating heart for the first time. This is achieved by a so-called ECG "trigger": ECG measures the heart function, so that SOMATOM 2 is synchronized with the patient’s heartbeat. Then, the device sends out X-ray pulses at a specific time point of the heart beating, and collects data during diastole instead of when the heart is pumping blood. This makes CT images largely free from the interference of heart activity.

SOMATOM 2,1979
Prospective ECG trigger sequence acquisition
Usually when we refer to the prospective ECG trigger scanning technology, we mainly refer to the prospective ECG trigger sequence acquisition.
At present, the prospective ECG trigger scanning technology has become the preferred cardiac imaging technology, which is exposed during the short and predetermined acquisition window of the cardiac cycle. The r wave on the electrocardiogram is monitored. Scanning starts after a time delay and stops after a time to resume at a similar time in the next cycle.
Early electron beam CT also used prospective ECG trigger scanning technology, which had high time resolution, but poor image quality, and was eventually eliminated (see). It can be seen that the image quality is in a very important position in imaging, and it is feasible to improve the temporal resolution in advance before ensuring the image quality.
Coronary CTA images of electron beam CT
Achenbach S . Value of electron-beam computed tomography for the noninvasive detection of high-grade coronary-artery stenoses and occlusions.[J]. New England Journal of Medicine, 1998, 339(27):1964.
The traditional prospective ECG trigger scanning technology is exposed at a specific time in the R-R interval, so the image quality will be reduced in the case of premature beats or other arrhythmia.
On 64-slice spiral CT, sequential scanning technique (about four exposures) is used to cover the whole heart. Skip one heartbeat between adjacent X-ray exposures to allow the patient table to move unless there is a low heart rate (for example, < 48 bpm), in which case the patient table can move during the X-ray stop time (systole). Due to the incorrect fusion of two adjacent data sets, staircase artifact is a shortcoming of traditional prospective ECG-triggered CTA. This may be caused by unstable heart rate and body movement. In this respect, 256-slice or 320-slice CT scanning, as well as the Flash mode of Shuang Yuan CT, allow scanning to be completed in one heartbeat, and there will be no cross-sectional artifacts.
At least 180 parallel ray projections are needed to reconstruct the image. Single-source CT scanner needs half a revolution plus a fan angle (about 50-60) to transmit such a large amount of data. The time resolution of the rotation center is half of the rotation time. In order to reduce the radiation dose as much as possible, the shortest gantry rotation (230–240) is used, and imaging is limited to one cardiac phase. In order to adapt to some heart rate changes or obtain wide-phase data (for example, end systole to end diastole), the exposure time can be extended at the expense of increasing radiation exposure.
The optimal duration depends on several factors:
1) the patient’s heart rate and variability;
2) the purpose of cardiac examination (coronary artery imaging or including functional analysis); and
3) Different gantry rotation speeds (0.25-0.35s/r) that affect the time resolution.
Different CT devices have different abilities to extend exposure time. If the exposure duration can be set long enough, functional imaging or multi-segment reconstruction using two adjacent cardiac cycles is possible.
In addition to the single-source CT scanner, for the first generation of Shuang Yuan CT, there are two acquisition systems installed on the rotating gantry with an angle offset of 90, and the 180 parallel ray geometric data can be divided into two 90 data segments. This 90 data segment was acquired at the same anatomical level at the same time. Therefore, the temporal resolution is 83 ms. When multi-sector reconstruction is applied, the temporal resolution of 41 to 83ms (60ms on average) can be achieved. For the new Shuang Yuan CT system, the time resolution of single sector can be improved to 66-75ms, and the highest time resolution can reach 33-37ms when multi-sector reconstruction is applied.
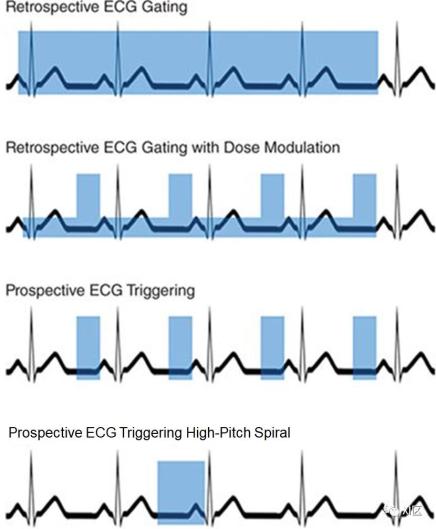
Gating/triggering technology. This picture shows four ECG gating/triggering methods, and the blue box shows the real-time current. In the case of retrospective ECG gating using dose modulation, the higher box represents the total tube current, while the shorter box represents the reduced tube current.
Prospective ECG trigger spiral acquisition
For Shuang Yuan CT system, a new forward-looking ECG-triggered spiral scanning technology (Flash Spiral mode) was invented. Flash Spiral mode and DSCT system provide a way to scan the heart in a heartbeat by using a new spiral acquisition (the examination table moves continuously during image acquisition) specially developed for DSCT.
In single source CT, the pitch must usually be limited to p≤1.5 to ensure seamless volume coverage along the Z axis. If the pitch is increased to p > 1.5, the appearance of sampling gap hinders image reconstruction, and there are not too many images to cause artifacts. For cardiac imaging, the pitch is generally around 0.2, and more overlap can ensure that the same phase position of different R-R intervals in the Z-axis direction is continuous. Interpolation artifacts will occur when the pitch is too large (see).
However, for DSCT, the data obtained by the second measurement system after a quarter of a week can be used to fill these gaps. In this way, the pitch can be increased to p > 3.2 while still allowing image reconstruction. The time resolution of each individual axial image is a quarter of the rotation time. At the same time, due to the high pitch, overlapping radiation exposure is avoided, thus reducing the radiation dose of patients to the minimum theoretically achievable, usually less than 1mSv.
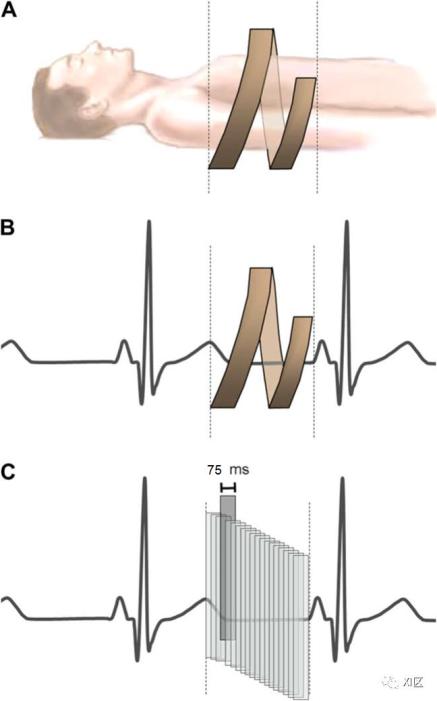
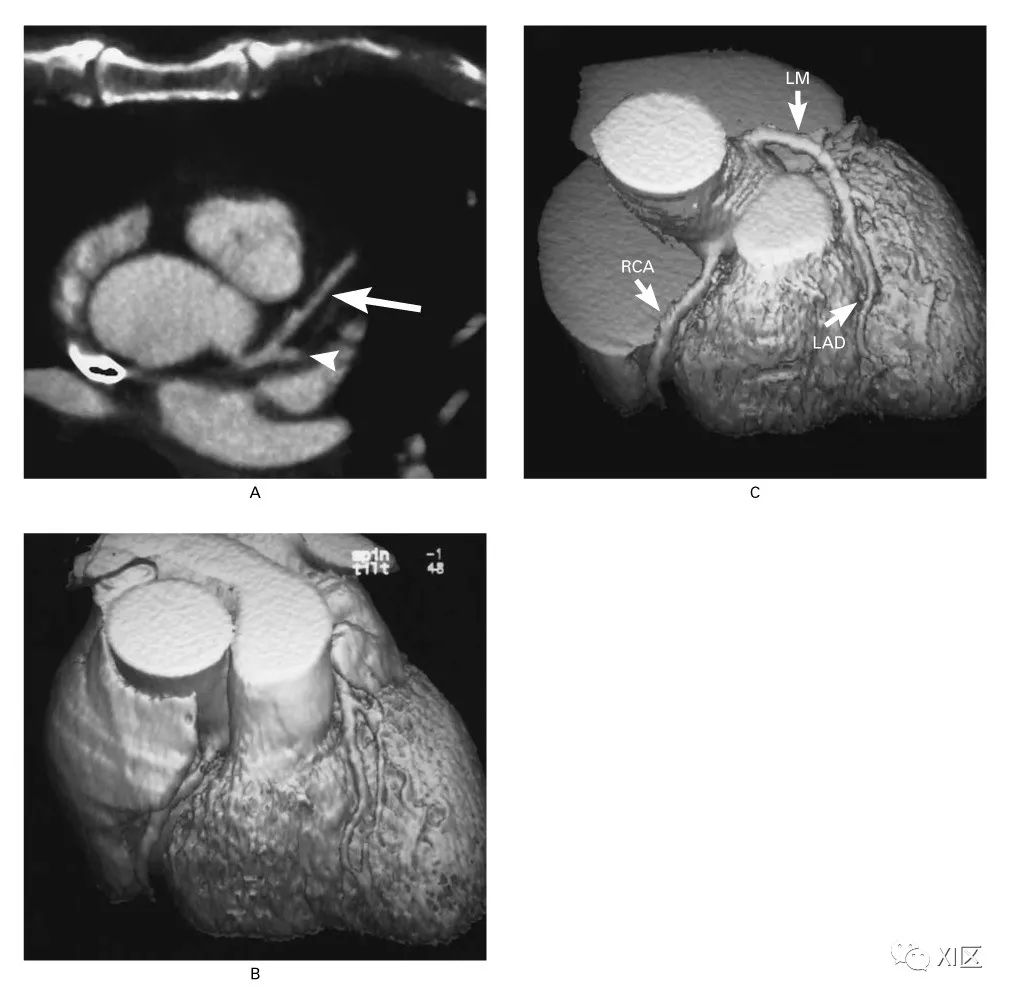
Schematic diagram of Flash spiral mode. For simplicity, only the path of one of the two groups of X-ray tubes and detectors is shown. (a) In the Flash spiral mode, a very high pitch is used so that the X-ray tube and detector can rotate around the patient without overlapping. (b) Image acquisition begins at the end of systole and is completed within one cardiac cycle. The actual duration of image acquisition depends on the width and scanning length of the detector. (c) The time resolution of image reconstruction is about one quarter of the gantry rotation time (here, the gantry rotation time is 280ms, and it is 75ms). Subsequent images are reconstructed at adjacent time points in the cardiac cycle.
Achenbach S, Marwan M, Schepis T, Pflederer T, Bruder H, Allmendinger T, Petersilka M, Anders K, Lell M, Kuettner A, Ropers D, Daniel WG, Flohr T. High-pitch spiral acquisition: a new scan mode for coronary CT angiography. J Cardiovasc Comput Tomogr. 2009 Mar-Apr; 3(2):117-21.
So let’s sum up, retrospective ECG is used in retrospective scanning, and then the reconstructed time image is determined according to ECG. Prospective scanning is ECG-triggered scanning, which can be divided into two modes, one is prospective ECG-triggered sequence scanning, and the other is prospective ECG-triggered spiral scanning, that is, large pitch mode, which can only be used in Shuang Yuan CT.
Therefore, the statement of "front door control" is untenable. To put it more strictly,